
Page 5 - Retiree News Fall 2020
P. 5
How to vote in New York
Below is is information for for CSEA members to to to help guide you you during the the COVID-19 Pandemic on on on on the the the best and and and safest way to to to to exercise your right to to to to VOTE on on on on November 3-Election Day CSEA encourages all members to to to participate in the the democratic process and and vote Absentee Ballot Application
New York
State has allowed the the use of of Absentee Ballots for November’s Election as as a a a a a a a a safe way to to vote due to to the the risk of COVID Any eligible voter can request request an an an absentee absentee ballot ballot TODAY!
Visit https://absenteeballot elections ny ny gov/ to request request an an an absentee absentee absentee ballot ballot ballot After receiving your your your absentee ballot ballot be be sure to to fill it out and and return postmarked no later than Election Day November 3 You may also hand deliver your your your your ballot ballot to to to your your your your county board of elections or to your early voting location Early Voting
Early Voting
period for this election will be be be October 24 – November 1 For information on on on where and when to early vote find
your county board of elections through this website https://cseany org/boe-links
Vote In Person
Election Day is November 3 Polls are open from 6 a a a a a a a a a m m m m to to 9 p p p p m m m m statewide that
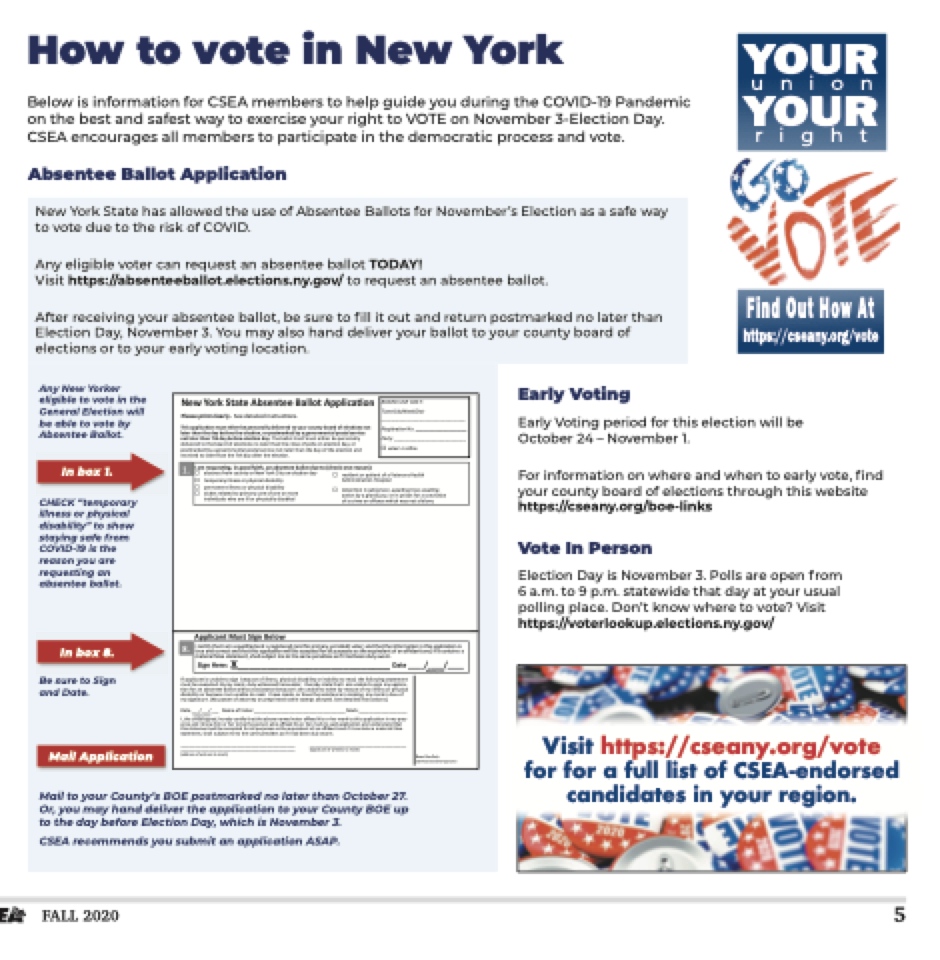
day at at at your usual polling place Don’t know where to to vote? Visit https://voterlookup elections ny gov/ Any New Yorker eligible to vote in the General Election will be able to vote by Absentee Ballot CHECK “temporary illness or or physical disability” to show staying safe from COVID-19 is the reason you are requesting an absentee ballot Be sure to Sign and Date New York
State !bsentee Ballot !pplication Please print clearly See detailed instructions/
BOARD USE ONLY: Town/City/Ward/Dist:
In box 1 resident or patient received no no later than the the the 7th day after the the the election/ !dministration Ho 1/
2/
2/
3/
4/ 3/
5/ 4/ 6/ 5/ 6/ temporary illness or or physical disability permanent illness or or physical disability I am requesting tin in in tin tin in good faith an an an an absentee ballot due to to (checkdoentenrtieoansoinnj)a:il/prison awaiting awaiting trial awaiting awaiting duties related to primary care of one or or or or or or more absence from county or or or or or New York
ity on on on election day action by a a a a a a a a a a a a a a a a a a grand jury or or or or in tin tin in prison prison for a a a a a a a a a a a a a a a a a a conviction resident or or or or patient of of o a a a a a a a a a a a a a Veterans Health individuals who are are ill ill or or or or or or or physically disabled temporary illness or or or physical physical disability of of o a a a a a a a a a a a a a crime or or or or offense which was not a a a a a a a a a a a a a felony !dministration Hospital
permanent illness or or or physical disability absentee ballot(s) requested for for the following election(s) detention in in tin tin in jail/prison awaiting awaiting trial awaiting awaiting duties related to primary care of one or or or or or more PirnidmivaidryuaElslewctihonaroenillyor physically disabledGeneral Election Election only only Special Election Election only only of o a a a a a a a a a crime or or or offense which was not a a a a a a a a a felony !nyelectionheldbetweenthesedates absencebegins _____/_____/_____ _____/_____/_____ absenceends _____/_____/_____ _____/_____/_____ lasbtsneamnteeoer sburanlalmote(s) requested for the following electiofinr(sst)na me Primary Election Election only only General Election Election only only MM/DD/YYYY
MM/DD/YYYY
middle initial suffix
!nyelectionheldbetweenthesedates absencebegins _____/_____/_____ _____/_____/_____ absenceends _____/_____/_____ _____/_____/_____ date of birth county where you live last name name or surname
MM/DD/YYYY
_____ _____ _____ /_____ /_____ /_____ /_____ address where you live (residenc dateofbirth MM/DD/YYYY
_____ _____ _____ /_____ /_____ /_____ /_____ Delivery of Primary Elec e) street apt county where you live tion allot (check one)
De
Delisvterereyt noof/ PrimsatreyetEnlaemcetion allot (check one)
Dealpivt/er to to me in pecritsyon at at at the the board board of of of elecsttiaotens zip code
I authorize (give name) _______________________________________ to to to to pick up my ballot ballot at at at at at the the the board board board of of of of of elections/ Delivery of of of of General (or Special) Election allot (check one)
Deliver to to to to me me me in in person at at at at the the the board board board of of of of elections elections elections Mail ballot to me me me at (mailing address)
I authorize (give name) _______________________________________ _______________________________________ _______________________________________ to to to to pick up my ballot ballot at at at at at the the board board of of of elections/ _______________________________________________________________________________________________________ stMreeatinl ob/allot sttoreemt neamate (mailing address)
apt/ city state
zip code
I authorize (give name) _______________________________________ to to to pick up my ballot ballot at at at at the the board of of of elections/ !pplicant Must Sign Below Mail ballot to me me at (mailing address)
_________________________________ BOARD USE ONLY: Registration No: ____________________ Town/City/Ward/Dist:
This application must either be be personally delivered to your county board of elections not New York
State !bsentee Ballot !pplication later than the the the the day before the the the the election election or or or postmarked by a a a a a a a a a a a a a a a a a a a a a a a governmental postal service nPolet alasterpthriant7ctlhedaarylyb efSoereedlecttiaoilnedaiyn sTthreubcatillont ist/self must either be be personally delivered to the the the board of of elections no later than the the the close of of polls on on on on on on on election election day or Tphoisstmapaprkliecdatiboynamgouvsetrenitmhenrtbael poesrtsaolnsaelrlvyicdelnivoetrleadtetrothyaonurthceoudnatyyobfotharedeolefcetlieocntiaonnds not not lraetcerivtehdanothlaetdear ythbaenfothre t7hteh edlaeyctiaoftne r r r r r r r r r r r r r r r r r r r r r r othr othr epoesletcmtiaornk/ed by a a a a a a a a a a a a a a a a a a a a a a a a a a a a a governmental postal service not not later than 7th day day before election day day The ballot itself must either be be be be personally deliverIeadmtortehqeubeosatirdngo f f f f f f f ienlegcotiondsfnaoitlha tearnthaabnsethnetecleosbeaollfoptodlluseontoel(ecchtieocnkdoany eoreason):
1/
postmarkedabsyeangceovferornmmceonutnatlyporstNael swerYvoicrke niotyt loanteerltehcatinonthdeadyay of the the the election election and Party: ____________________________ ____________________________ _________________________________ voted in office Registration No: ____________________ Party: ____________________________ voted in office of of a a a a Veterans Health spital
action by a a a a a a a a a a a a a a grand jury or or or in tin tin in prison prison for a a a a a a a a a a a a a a conviction Special Election only MM/DD/YYYY
MM/DD/YYYY
MM/DD/YYYY
MM/DD/YYYY
phone number (optional) email (op (op first name city phone number (optional) liver to to me in person at the address where you live live live (residence) street apt city state
zip code
I authorize (give name) _______________________________________ to to to pick up my ballot ballot at at at at the the board board of of of elections/ Mail ballot to me me at (mailing address)
_______________________________________________________________________________________________________ tional) middle initial zip co state
email (optional) NY board board of elections suffix
de NY 7/
7/
Delisvterereyt noof/ Genestraeelt(noarmSepecial) Election allot (check one)
apt/ Delivercityo me me me in person at at at at the the bstoaaterd of of of elezcipticodnes
________________________________________________________________________________________________________
In box 8 8/
I I c_e_r_t_if_y_t_h_a_t_I_a_m__a_q__u_a_li_fi_e_d_a_n_d__a__re_g_i_s_te_r_e_d__(a_n_d__f_o_r_p_r_im__a_r_y_ e__n_ro_l_le_d_)__vo__te_r_-_a_n_d__th_a_t__th_e__in_f_o_r_m__a_ti_o_n_i_n_t_h_i_s_a_p_p_l_ic_a_ti_o_n__is_
street street no/ street street name apt/ true and and and correct and and and that
this application will be be accepted for all all purposes as as the the equivalent of an an an an an affidavit and and and if if if it it it contains a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a city state
zip code
material false statement shall subject me me me to the the same penalties as as if I had been duly sworn/
!pplicant Must Sign Sign Below Sign Sign Here: X__________________________ Date ____/____/____ I I certify that
that
that
I I am a a a a a a a a a a a a a a a a a a a a a a a a a a a a a qualified and and and and and and a a a a a a a a a a a a a a a a a a a a a a a a a a a a a registered (and for for for primary enrolled) voter- and and and and and and that
that
that
the the information in in in tMhMis/DaDp/YpYYliYcation is is is is 8/
true and and and and and and correct and and and and and and that
that
that
this application will be accepted for for for all purposes as as as the the the equivalent of an an an an an an an an an affi vit and and and and and and if if if if it it it it contains a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a If applicmanateisriuanl faablsletsotastigenmebnetc asuhsaellosfuilblnjecsts mpehytsoictahledsisaambielitpyeonrailntiaebsilaitsyiftoI hreaaddb etheenfdoullloywsiwngorsnta/ tement must be executed y my my mark duly witnessed hereunder I I I I I hereby state
that
I I I I I am am am unable to to to sign my my applica-
X _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ tion for aSnigabnseHntereeb:all
disability or or or or or or because I I I am am am am unable to to tto read/ I I I have have made or or or or or or have have the assistance in in in in in making my my mark in in in in in lieu of of ot w it hou
ta ssi sta nc eb eca us eI
am un ab le to wr
my my signature/ (No power of of attorney or or or or or preprinted name stamps allowed/ See detailed instructions/)
If applicant is is unable unable tto to to to sign sign sign because of of illness physical disability or or or inability tto to to to read the following statement must be be be executed y my my my mark duly witnessed hereunder I I I I hereby state
state
that
I I I I am am am unable unable unable to to to to sign sign my my my applica-
Date ___/___/___ Name of of Voter ____________________________________ Mark ___________________ ___________________ tion for an an absentee ballot without assistance because I I I I I am am am am unable unable to to to write by by reason of of my my my my illness or or or or or physical MM/DD/YYYY
dI itshaebiulintydeorrsibgenceadu sherIeabmy cuenratibfylethtoatrtehaeda/bIohvaevneamaedev ooterrhaffivexethdehiassosirshtaenrcmeairnkmtoatkhinisga pmpylicmatiaorkniin lmieyuporfes- menycesiagndatIukrneo/w(Nhoimpowrehrerotfoabtteotrhneypeorsponrewprhiontaeffidxneadmheissotrahmeprsmaallrokwtoedsa/iSdeaepdpelitcaitileodniannsdtrunctideornsst/a)ndthat this statement will be accepted for all all purposes as the equivalent of of an an an affidavit and if if it i it it contains a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a material false sDtatem__e_n/t _s_h_a/l_l s_u_bjeNcatme otof Vthoetesra m__e_p_e_n_a_l_ti_e_s _a_s _if_I_h_a_d__b_ee_n__d_u_ly__sw__o_rn_/_____ Mark ___________________ MM/DD/YYYY
I I the the the undersigned hereby certify that
that
the the the above named voter affixed affixed his his his or or or her her her her mark mark to to to this application application in my pres- _____________________________________________ _____________________________________________ ______________________________________ ______________________________________ ______________________________________ ence and and and and I I know him or or or or her her her her to to to to be be the the the the person who affixed affixed his his his his or or or or her her her her mark mark mark to to to to said application application and and and and understand that
that
_____________________________________________ _____________________________________________ (signature of of of witness witness to to to to mark)
mark)
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ ite by rea _ _ _ _ _ _ _ _ _ so _ _ _ no fm
_ _ _ _ _ _ y y illn ess MM/DD/YYYY
Board Use Only
2020 Absentee Ballot Application
_ _ _ _ _ _ _ _ or pDhaysticeal_ __/____/____ Mail Application
this statement statement will be be be accepted for all all purposes as as the the the equivalent of of of an an an an an affidavit and and and and if if it it it it contains a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a material false (address of witness to mark)
statement statement shall subject me me me me to to the the same penalties as as if I had been duly sworn/
_____________________________________________ _____________________________________________ ______________________________________ ______________________________________ ______________________________________ _____________________________________________ _____________________________________________ (address of witness to mark)
(signature of witness to mark)
da _ _ _ Board Use Only
2020 Absentee Ballot Application
Mail to to to your your County’s BOE BOE postmarked no later than October 27 Or you you you may hand deliver the the application to to to to your your County County BOE BOE up to to the the day before Election Day which is November 3 CSEA recommends you submit an application ASAP Visit https://cseany org/vote for for for for a a a a full list of CSEA-endorsed candidates in your region FALL 2020 5 YOUR
YOUR
union YOUR
YOUR
right Find Out How At https://cseany org/vote 